
Surgical face masks and filtering respirators are standardized protective gear that accommodate a wide variety of users; they ought to fit any body. Even though these devices were designed as universal and seemingly neutral, they cling to specific bodies differently and signal gendered aspects of care work and vulnerability amidst the COVID-19 outbreak. The embodied gender differences might not be revealed directly in the materiality of the mask itself, but remain deeply coded in the guidelines of use and visual representations of this anti-epidemic technology.
While surgical masks and cloth face-coverings serve as a loose-fitting barrier between the user’s face and the external environment, the N95-type respirators require a very close facial fit to properly seal off the mouth and nose and ensure efficient filtration. As such, properly fitting the respirator might pose a problem for persons with facial hair because it can interfere with its sealing surface. For this reason, in 2017 the U.S. National Institute for Occupational Safety and Health (NIOSH) of the Center for Disease Control and Prevention (CDC) issued a chart that catalogs various beard and moustache styles according to their suitability for workers who regularly wear tight-fitting respirators.
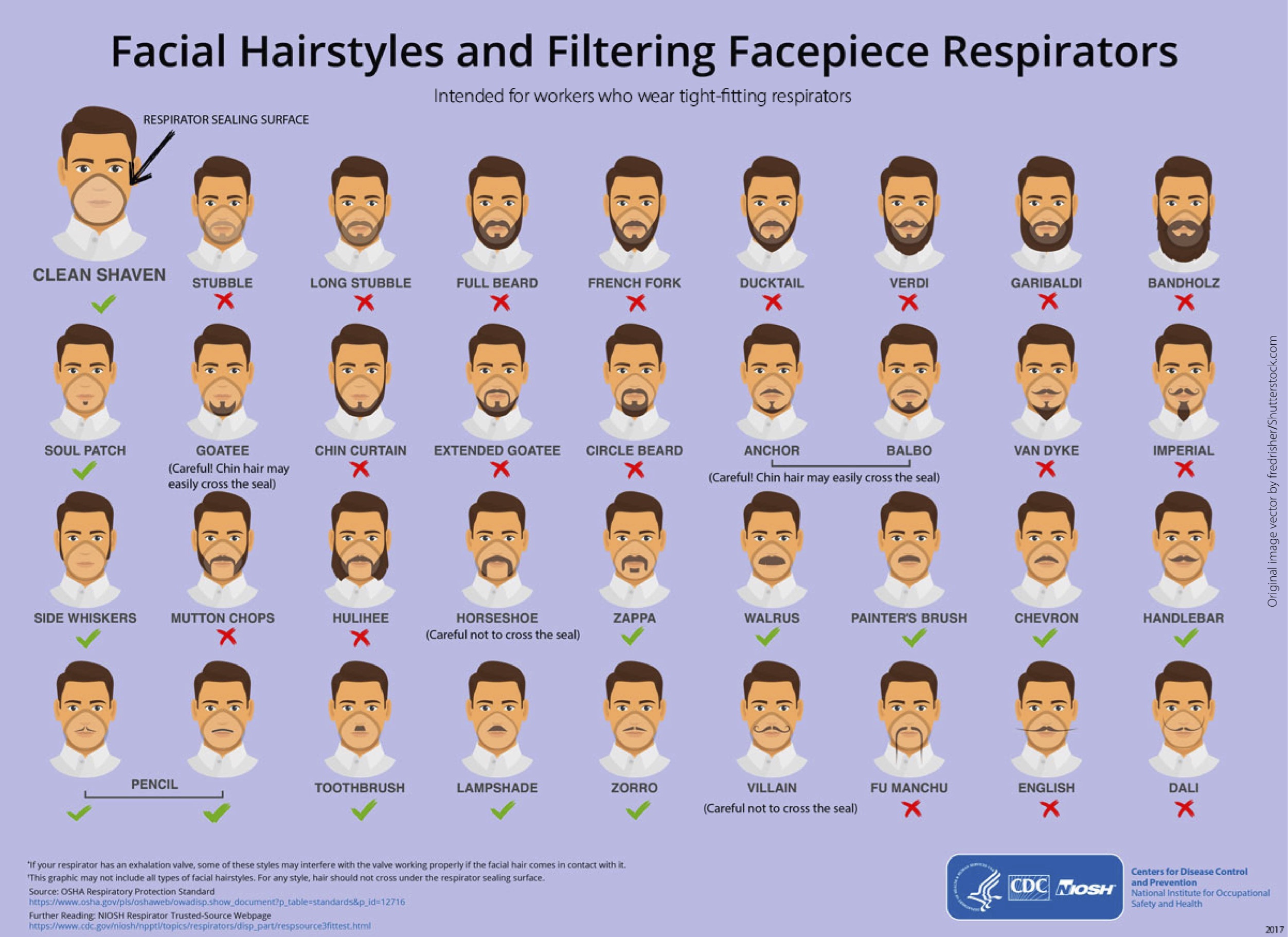 Image Source: Center for Desease Control
Image Source: Center for Desease Control
While sporting a soul-patch, Zorro or Zappa moustache should be fine, mutton chops, chin curtain, and French fork beard are not recommended. Sometimes the human body needs to adapt to the mask, not the other way around. This humorous infographic contains an important message for ensuring safety of the medical staff, especially given that the latest research on the development of the COVID-19 pandemic shows that men are more vulnerable to infection than women.1
At the same time, women make up 70 percent of the global healthcare workers that are at greatest risk. According to the WHO Health Workforce Department, “women comprise seven out of ten health and social care workers and contribute US$ 3 trillion annually to global health, half in the form of unpaid care work.”2 This means that the vast majority of primary users of medical face masks and respirators are female nurses, residents, and doctors. The current coronavirus pandemic puts their bodies on the frontline. Healthcare workers across the U.S. and Europe are protesting the critical lack of Personal Protection Equipment (PPE) with messages such as: “Don’t send us to battle without weapons! Get me PPE!”. Adopting this kind of military vocabulary that presents the counter-epidemic technology as weaponry against the invisible enemy, echoes the historical context in which some of the first modern respirators were developed, namely, the chemical warfare of the First World War. Even prior to this major stimulus for engineering better respiratory devices to protect soldiers against chlorine, phosgene, and mustard gas in combat, modern respirators were designed for other male-dominated professions, specifically for miners and firefighters, whose working conditions expose them to hazardous dusts, smoke, and carbon monoxide. Just like with most other modern technologies and medical models, their assumed user is a “Reference Man” that is hailed to represent all humanity. In other words, respirators were designed for male bodies in industrial settings and warfare. This stands in stark contrast to care work performed by predominantly female medical personnel battling the coronavirus pandemic at the moment.
But does this history make any difference for contemporary designers and users? Would a respirator modeled on a female body look or function differently? According to a scientific paper on pregnant users of N95 masks, “filtering facepiece respirators developed to meet the respiratory limitations of pregnant wearers might offer a universal design that would improve the comfort and tolerability for all users.”3 Perhaps this perspective and retiring the “Reference Man” could help in designing better equipment for all. Certified facepiece masks are tested for their biocompatibility, or an “ability to be in contact with a living system without producing an adverse effect.”4 This scientific term is typically used to describe the interaction between a biomaterial (for example one used in protheses or implants) and the human body. Even though the face mask is not corporally-integrated in the same way as artificial joints or pacemakers are, it serves as an extension of the body and becomes part of the biological respiratory system. Face masks and respirators come in different sizes but, apart from this variation, their basic form remains the same for differently-gendered bodies. It is the discourse and iconography around the use and availability that is often gendered. Treating a mask as an extension of the body helps to see through different layers of the functionality that this artifact holds for different users.
The performative capacity of the face mask as a lifesaving device can even extend beyond the physical materiality and functionality of the artifact itself. The metonymical face mask is featured in the “Mascarilla-19” campaign launched by the Canary Islands Institute for Equality to combat another global pandemic, that of gender-based violence. This time the mask functions as a code word: asking for a “Mask-19” at a pharmacy allows women who experience abuse or sexual assault to access help. Restricted movement and social distancing rules under lockdown bear gendered consequences, with a reported surge in domestic violence cases. As home is not always a safe space for women, the symbolic mask is being mobilized to save lives. The campaign has started to spread to other Spanish provinces and was also adopted in France. The mask is a powerful symbol: the most desired and inconspicuous object, that quickly became part of everyday life around the globe, helps women who experience violence to voice something that might be difficult to admit and escape.
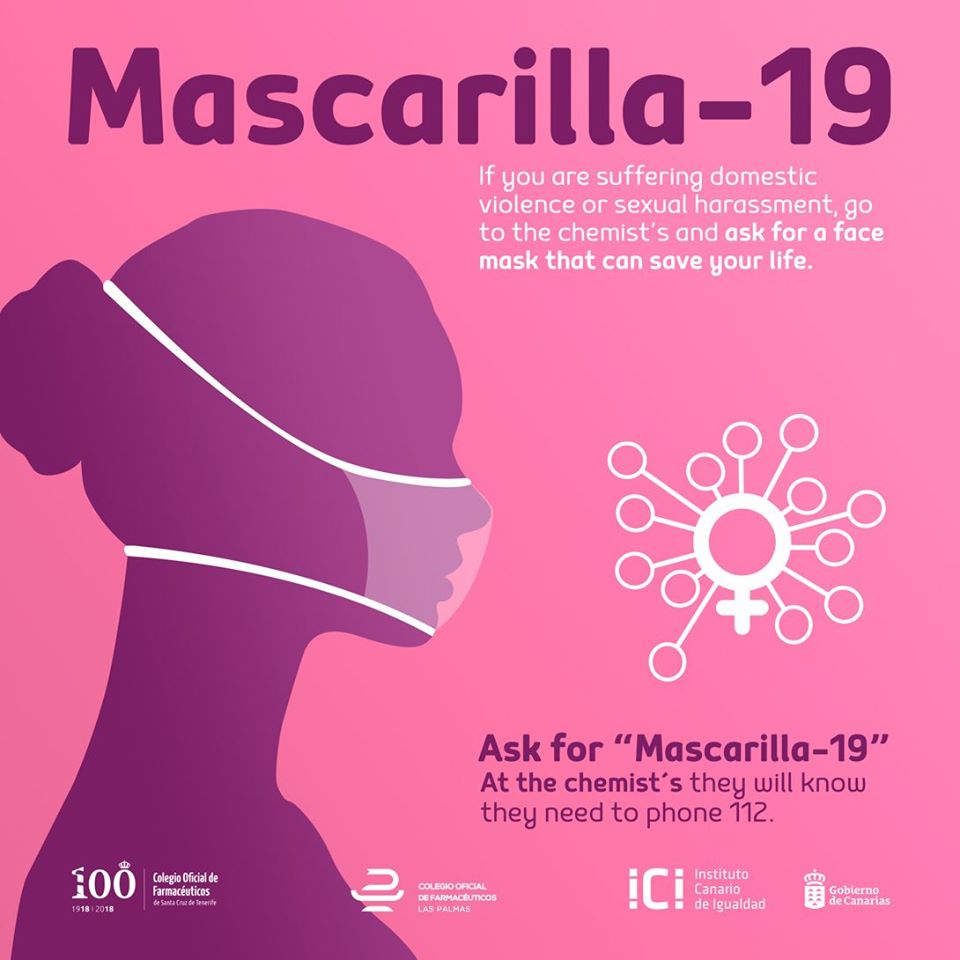 Image source: Gobierno de Canarias
Image source: Gobierno de Canarias
The idea that faces behind masks are equal can be misleading. In the current COVID-19 crisis, public health experts highlight the importance of keeping track of sex-disaggregated data, but also of gendered behavioral patterns (such as smoking or diet) that can affect immunity.5 Whether it comes to higher fatality rates, design and distribution of lifesaving technologies, or labor regimes of care, gender is one of the key factors that make certain bodies more vulnerable than others during health crises.
About the author: Marianna Szczygielska is Postdoctoral Fellow at the Max Planck Institute for the History of Science in Berlin where she works on human-animal relations and materialities. A feminist researcher, she also looks into the gendered aspects of artifacts, technologies, and practices that we encounter in our daily lives.
References:
1 Nanshan Chen et al., “Epidemiological and Clinical Characteristics of 99 Cases of 2019 Novel Coronavirus Pneumonia in Wuhan, China: A Descriptive Study,” The Lancet 395, no. 10223 (February 15, 2020): 507–13.
2 Boniol M, McIsaac M, Xu L, Wuliji T, Diallo K, Campbell J. “Gender Equity in the Health Workforce: Analysis of 104 Countries.” Working paper 1. Geneva: World Health Organization; 2019 (WHO/HIS/HWF/Gender/WP1/2019.1). Licence: CC BY-NC-SA 3.0 IGO.
3 Raymond Joseph Roberge, “Physiological Burden Associated with the Use of Filtering Facepiece Respirators (N95 Masks) during Pregnancy,” Journal of Women’s Health 18, no. 6 (June 1, 2009): 819–26.
4 Michel Vert et al., “Terminology for Biorelated Polymers and Applications (IUPAC Recommendations 2012),” Pure and Applied Chemistry 84, no. 2 (January 11, 2012): 381.
5 Clare Wenham, Julia Smith, and Rosemary Morgan, “COVID-19: The Gendered Impacts of the Outbreak,”The Lancet 395, no. 10227 (March 14, 2020): 846–48.
Image credit: Nurse with mask in the Spanish flu ward 1918. Walter Reed. Harris & Ewing photographers / Public domain